The job description, if anyone had bothered to write one, would have been alarming. Stand between an enraged bull and a thrown cowboy. Distract the animal. Get the rider clear. Do it in under six seconds, in front of ten thousand people, with no protective equipment worth mentioning and a first-aid kit that was mostly hope.
And then do it again at the next show.
For the rodeo clowns and arena medics of the 1940s, 1950s, and 1960s, this was just Tuesday. And in the process of surviving it, they built something that American medicine is still using today.
The Arena as Laboratory
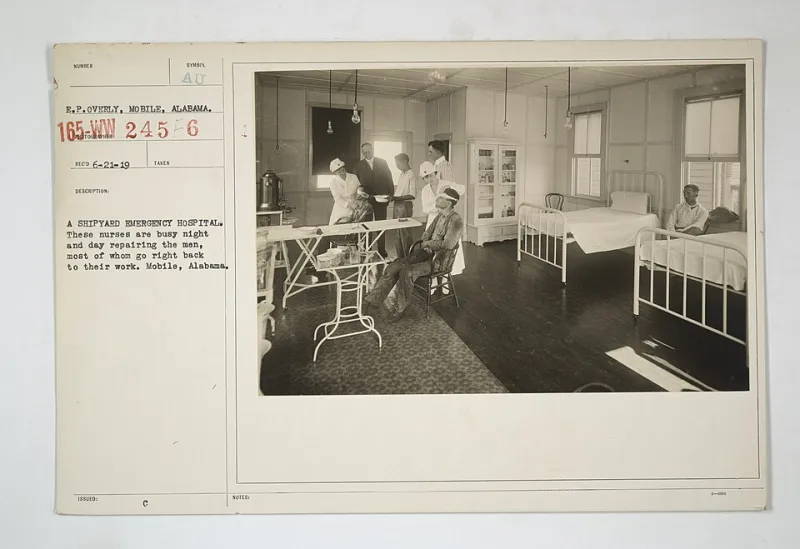
Modern emergency medicine, as a formal specialty, didn't exist until 1968, when the American College of Emergency Physicians was founded. Before that, emergency care was largely improvised — a patchwork of general practitioners, surgical residents, and whoever happened to be nearby when something went wrong.
 Photo: American College of Emergency Physicians, via nwtmediagroup.com
Photo: American College of Emergency Physicians, via nwtmediagroup.com
In rodeo, "whoever happened to be nearby" was usually a man in face paint and baggy overalls.
The rodeo circuit of midcentury America was a genuinely dangerous environment. Professional bull riding, bareback bronc riding, and steer wrestling produced injuries at a rate that would horrify a modern occupational safety inspector. Broken bones were routine. Internal injuries were common. And the time between injury and intervention was measured in seconds, not minutes, because the alternative was getting trampled.
This created a pressure that no hospital training program could replicate: the absolute necessity of making the right call immediately, with limited tools, in a chaotic environment, while something very large and very angry was still in the vicinity.
Out of that pressure came some genuinely revolutionary thinking.
The Men in the Barrel
Figures like Quail Dobbs, Homer Holcomb, and a lesser-known circuit regular named Earl "Dusty" Hargrove became legendary in rodeo circles not just for their crowd work but for their almost supernatural ability to assess and manage injured riders in the seconds after a fall.
Hargrove, who worked the southwestern circuit from the late 1940s through the early 1960s, was particularly influential. A former Army medic who had served in the Pacific, he brought military field medicine instincts into the arena and adapted them to the specific mechanics of rodeo injury — which, it turned out, had its own patterns.
Bull riding injuries concentrated in predictable anatomical zones. The sequence of events in a bad ride — the dismount, the fall, the secondary contact — produced injury combinations that Hargrove began cataloguing on index cards he kept in his costume pockets. After a decade on the circuit, he had a working taxonomy of rodeo trauma that no medical school had come close to assembling.
More importantly, he had protocols. Not written ones — Hargrove wasn't a bureaucrat — but deeply ingrained physical sequences: how to approach a downed rider, what to check first, how to move someone with a potential spinal injury when the alternative was leaving them in the path of a bull, how to manage airway obstruction with the tools available in a rodeo first-aid kit circa 1955.
Those protocols spread the way all informal knowledge spreads: person to person, circuit to circuit, show to show.
The Language Nobody Was Speaking
What makes the rodeo medicine story genuinely strange is how long it took the formal medical establishment to notice what was happening in the arenas.
The core insight that Hargrove and his peers had developed — that effective emergency response required a standardized sequence of assessment and intervention performed rapidly under stress — was essentially the same insight that would eventually produce Advanced Trauma Life Support (ATLS) protocols in the late 1970s. The ATLS system, now the global standard for trauma care, teaches physicians to follow a structured primary survey: airway, breathing, circulation, disability, exposure. In that order, every time, regardless of what the injury looks like.
Rodeo medics were doing something functionally identical, for functionally identical reasons, twenty years earlier. They just didn't call it anything. They called it staying alive.
The connection between arena medicine and formal trauma protocol development isn't perfectly documented — history rarely is when the innovators are working-class performers rather than academic physicians. But several of the physicians involved in early trauma system design in the 1960s and 1970s, including some who worked with the emerging network of trauma centers in Texas and Oklahoma, had direct exposure to rodeo medicine culture. A few had served as arena physicians on the circuit before moving into hospital practice.
The ideas traveled with them.
Chaos as Curriculum
What the rodeo arena offered that no simulation could replicate was genuine, uncontrolled chaos — the kind that strips away everything except what actually works.
Hospital emergency medicine, even in its early years, operated within a structure: walls, equipment, colleagues, time. Rodeo medicine operated in the space between a bull's horns and a dirt floor, with a crowd screaming and a clock running and no one to call for backup.
That environment was brutal. It was also clarifying in a way that structured training environments struggle to achieve. You couldn't rely on equipment you didn't have. You couldn't wait for a specialist who wasn't coming. You had to know, in your body, what to do first — and the consequence of getting it wrong was immediate and visible.
The physicians who eventually formalized trauma care were working toward the same clarity from the opposite direction: trying to strip hospital protocol down to its essential core, to find the sequence that worked when everything else was stripped away. The rodeo men had already found it. They'd just found it the hard way.
What the Clowns Left Behind
The rodeo clown as a figure in American culture is almost purely comic — the pratfalls, the barrel, the oversized shoes. The image is so thoroughly absurd that it tends to swallow the reality of what these men were actually doing.
They were first responders operating in one of the most dangerous occupational environments in the country, inventing emergency medicine protocols in real time because nobody else was going to do it for them.
The greasepaint was the costume. The work underneath it was deadly serious.
Modern emergency medicine acknowledges a lot of debts — to military medicine, to disaster response, to the trauma surgeons of the Vietnam era. The debt to the rodeo circuit is quieter, less documented, and almost never mentioned in medical school curricula.
But somewhere in the logic of every trauma bay — in the discipline of the primary survey, in the insistence on sequence over instinct, in the understanding that chaos requires structure more than calm does — there's a little bit of Dusty Hargrove, working the crowd and watching the gate and knowing exactly what he'll do when the ride goes wrong.
Because it always goes wrong. And you'd better already know.